


 Sign Out
Sign Out

In the heart nifedipine dilates the coronary arteries, especially the large conductance vessels, even in the free wall segment of partially stenosed areas. Further, nifedipine reduces the vascular smooth muscle tone in the coronary arteries and prevent vasospasm. The end-result is an increased poststenotic blood flow and an increased oxygen supply. Parallel to this, nifedipine reduces the oxygen requirement by lowering peripheral resistance (afterload). With long-term use nifedipine can also prevent the development of new atherosclerotic lesions in the coronary arteries.
Nifedipine reduces the smooth muscle tone of the arterioles, thus lowering the increased peripheral resistance and consequently the blood pressure.
At the beginning of the nifedipine treatment there may be a transient reflex increase in heart rate and thus in the cardiac output. However, this increase is not enough to compensate for the vasodilation. In addition nifedipine increases sodium and water excretion both in the short-term and long-term use. The blood-pressure-lowering effect of nifedipine is particularly pronounced in hypertensive patients.
Pharmacokinetics: Niferin SR 30mg tablets are formulated to provide nifedipine at an approximately constant rate over 24 hours. Nifedipine is released from the tablet at a zero-order rate by a membrane-controlled, osmotic push-pull process. The delivery rate is independent of gastrointestinal pH or motility. Upon swallowing, the biologically inert components of the tablet remain intact during gastrointestinal transit and are eliminated in the faeces as an insoluble shell.
Absorption: After oral administration nifedipine is almost completely absorbed. The systemic availability of orally administered nifedipine immediate release formulations (Nifedipine capsules) is 45 to 56 % owing to a first pass effect. At steady-state the bioavailability of Nifedipine tablets ranges from 68 to 86% relative to Nifedipine capsules. Administration in the presence of food slightly alters the early rate of absorption, but does not influence the extent of drug availability.
Plasma drug concentrations rise at a controlled rate after Nifedipine dose and reach a plateau at approximately 6 to 12 hours after the first dose. Following multiple days of dosing, relatively constant plasma concentrations at this level are maintained with minimum peak to trough fluctuations over a 24 hours dosing interval (0.9 to 1.2ng/mL).
Table: Peak plasma concentrations (Cmax) of Nifedipine tablets and the time to reach the peak plasma concentrations (tmax): (See table.)
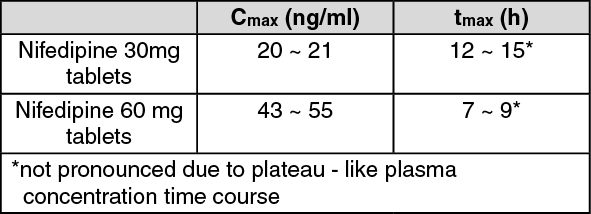 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageDistribution: Nifedipine is about 95 % bound to plasma protein (albumin). The distribution half-life after intravenous administration has been determined to be 5 to 6 minutes.
Biotransformation: After oral administration nifedipine is metabolised in the gut wall and in the liver, primarily by oxidative processes. These metabolites show no pharmacodynamic activity.
Nifedipine is excreted in the form of its metabolites predominantly via the kidneys, and about 5 to 15 % via the bile in the faeces. The unchanged substance is recovered only in traces (below 0.1 %) in the urine.
Elimination: The terminal elimination half-life is 1.7 to 3.4 hours in conventional formulations (Nifedipine capsules). The terminal half-life after Nifedipine Tablets does not represent a meaningful parameter as a plateau- like plasma concentration is maintained during release from the tablets and absorption. After release and absorption of last dose, the plasma concentration finally declines with an elimination half-life as seen in conventional formulations.
In cases of impaired kidney function, no substantial changes have been detected in comparison with healthy volunteers.
In cases of impaired liver function, the total clearance is reduced. A dose reduction may be necessary in severe cases.